What Is the Norwood Scale and Why Does It Matter for Your Hair Transplant?
If you’ve spent any time researching hair transplants, you’ve almost certainly encountered references to the Norwood scale — the classification system used to describe the progression of male pattern hair loss. Clinics reference it in consultations. Before-and-after galleries organize results by Norwood type. Surgical planning discussions use it as a shared language for describing how much hair loss a patient has and where it is.
But many patients who encounter the Norwood scale in research don’t fully understand what it measures, what its limitations are, and why it matters specifically for how their procedure is planned. Knowing your Norwood type is useful as a rough map of where you are in the hair loss progression. Understanding what the scale actually tells you — and what it doesn’t — is what allows you to engage meaningfully with the surgical planning conversation rather than simply receiving a number.
This guide explains the Norwood scale in full: its origins, its structure, what each type looks like, why it matters for hair transplant planning, and where it falls short as a planning tool — because the clinical picture of any individual patient is more complex than any classification system can fully capture.
The Origins of the Norwood Scale
The Norwood scale was developed by Dr. James Hamilton in the 1950s, who created an initial classification of male pattern baldness based on his observations of hair loss patterns in a large population of men. The scale was subsequently revised and expanded by Dr. O’Tar Norwood in the 1970s, whose name the scale now carries.
Norwood’s revision added additional types and subtypes that more accurately described the range of male pattern hair loss presentations he encountered in clinical practice. The resulting Norwood-Hamilton scale — typically abbreviated to simply the Norwood scale — became the standard classification system used by hair restoration surgeons worldwide, a position it has maintained for over fifty years.
The scale’s longevity reflects its practical utility: it provides a shared vocabulary that allows surgeons, researchers, and patients to communicate about hair loss patterns without needing to individually describe each patient’s presentation from scratch. Its limitations are equally well-established, and experienced surgeons understand it as a useful starting framework rather than a precise clinical descriptor.
The Norwood Scale: Each Type Explained
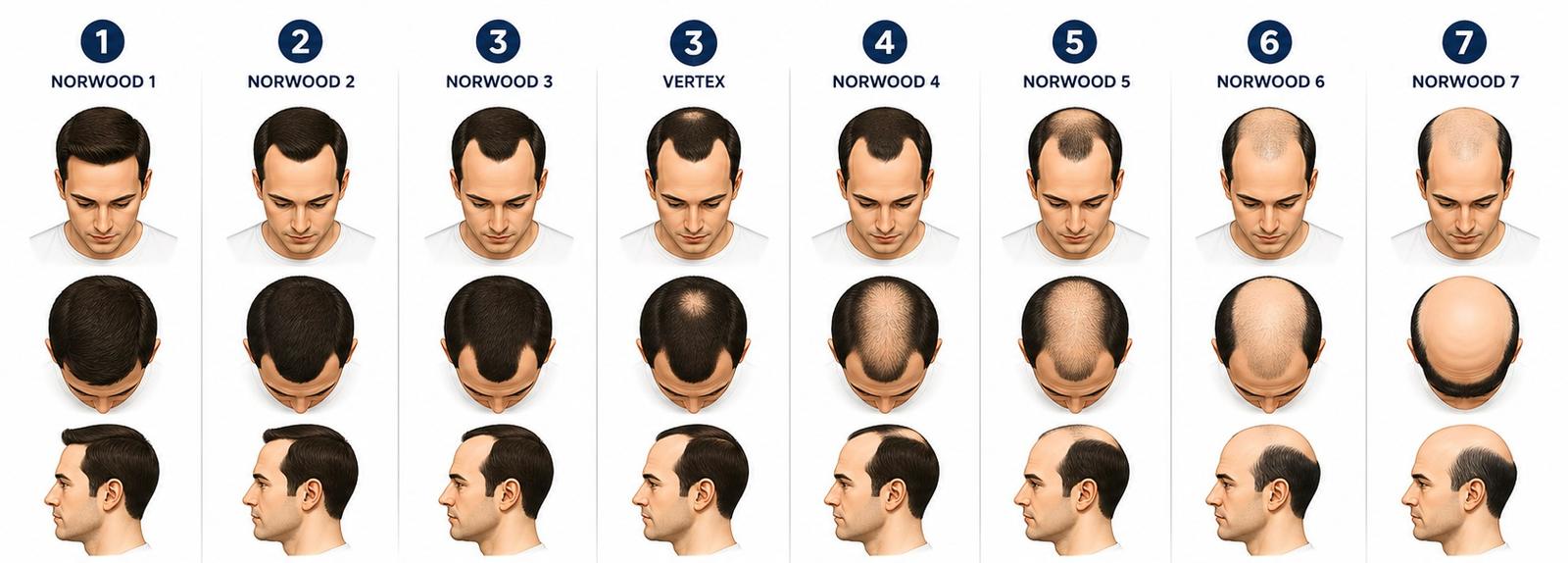
The Norwood scale runs from Type 1 through Type 7, with several types having variants that capture presentations that don’t fit neatly into the main sequence.
Norwood Type 1 represents no significant hair loss — the hairline is intact, sitting in its natural juvenile or mature adult position with no meaningful recession. Type 1 is essentially the baseline: normal hair with no evidence of androgenetic progression. Most men who are classified as Type 1 are seeking assessment rather than treatment, and surgical intervention is rarely indicated at this stage.
Norwood Type 2 shows slight recession at the temples — the first visible sign of androgenetic progression. The hairline has begun retreating at the corners, but the recession is relatively minor and the overall frontal hairline remains largely intact. Type 2 patients often notice the change in photographs or under specific lighting conditions before it becomes obvious in daily interaction. This is frequently the stage at which younger patients first present for consultation, having noticed the beginning of a process they want to address proactively.
Norwood Type 3 represents more defined recession at the temples, with the recession having deepened to form the characteristic M-shape that many people associate with the early stages of significant hair loss. The frontal hairline has retreated noticeably, and the temples are thinning or absent in the recessed zones. Type 3 is the most common stage at which patients present for their first consultation and first procedure, as the visual change has become sufficiently apparent to motivate action.
The Type 3 Vertex variant — sometimes written as Type 3A or Norwood 3V — describes a pattern where significant loss is occurring primarily at the crown (vertex) rather than, or in addition to, the temples. Some patients develop crown loss early in their progression and relatively limited frontal recession — a pattern that is clinically important because it requires different planning priorities than the standard Type 3 presentation.
Norwood Type 4 describes a pattern where both frontal recession and crown thinning have advanced significantly. The hairline has retreated further, the temples are more extensively lost, and a zone of thinning or loss at the crown is clearly established. The area of retained hair between the frontal loss and the crown loss — the mid-scalp bridge — is becoming narrower. Type 4 patients typically require more comprehensive coverage planning than Type 3 patients, and the consultation must address both the frontal zone and the crown rather than focusing exclusively on the hairline.
Norwood Type 5 represents a further stage of progression where the separation between the frontal zone of loss and the crown zone of loss has narrowed further, with the mid-scalp bridge becoming increasingly thin. The overall area of loss is substantially larger than Type 4, and the planning considerations shift accordingly — the donor supply must be allocated across a larger recipient area, which affects both the density achievable in any given zone and the number of sessions likely to be required across the patient’s lifetime.
Norwood Type 6 describes a pattern where the frontal and crown zones of loss have merged — the mid-scalp bridge has been lost, creating a single large expanse of loss across the top of the scalp. What remains is the horseshoe pattern of retained hair at the back and sides of the scalp that characterizes advanced androgenetic alopecia. At Type 6, the total recipient area is large and the planning conversation must be very explicit about what is achievable within the donor supply, what coverage is prioritized, and what realistic expectations should include.
Norwood Type 7 is the most advanced classification — extensive loss that extends into the sides of the horseshoe, with the remaining hair band becoming narrower and lower. The permanent donor zone is more limited at Type 7 than at earlier stages, the recipient area is at its maximum extent, and the gap between what can be transplanted and what would be needed for comprehensive coverage is at its largest. Type 7 patients can achieve meaningful improvement through transplantation, but the consultation must be very honest about the trade-offs involved in allocating limited donor supply across a very large area of loss.
The Type A Variants
The Norwood scale includes a set of variant classifications — designated with the letter A — that describe a different pattern of hair loss progression from the main sequence.
In the standard Norwood progression, recession typically advances from the temples back while crown loss develops separately, with the two zones of loss eventually merging. In the Type A variant pattern, recession progresses differently — advancing uniformly from the front to the back without the characteristic mid-scalp bridge of retained hair that separates frontal and crown loss in the standard pattern.
Type 2A, 3A, 4A, and 5A describe progressively advanced versions of this alternative progression pattern. Patients with Type A variants have a different distribution of loss than patients with the equivalent numeric type in the standard sequence, and the surgical planning implications can differ accordingly. A Type 4A patient may have different priorities than a Type 4 patient with the standard pattern, because the distribution of loss is different even if the overall severity is similar.
Why the Norwood Scale Matters for Hair Transplant Planning
The Norwood scale is clinically relevant to hair transplant planning in several specific and interconnected ways that go beyond simply having a label for the degree of loss.
It shapes the coverage conversation. The total area of loss — and how it’s distributed across the scalp — directly determines how many grafts are needed to achieve a given density across that area, what zones need to be prioritized, and what can realistically be achieved with the available donor supply. A Type 2 patient and a Type 6 patient are having fundamentally different conversations about what a procedure can accomplish, and the Norwood classification is the starting point for understanding why.
It informs donor supply planning. Higher Norwood types require more grafts to address the existing loss — and in patients where loss is still progressing, the future loss pattern will likely follow the trajectory suggested by the current Norwood classification and family history. A Type 3 patient whose father and grandfather are Type 6 is almost certainly planning for a Type 5 or 6 eventual pattern, which means the donor supply management conversation must account for a much larger lifetime recipient area than the current Type 3 presentation suggests.
It guides hairline design decisions. The appropriate hairline position and design varies with Norwood type in ways that are not always intuitive. A Type 2 patient getting a hairline transplant can afford a relatively forward, complete-looking hairline because the surrounding native hair provides good context and the pattern may not progress dramatically further. A Type 4 or 5 patient getting frontal work needs a hairline designed with explicit awareness of the thinning mid-scalp behind it — a complete-looking hairline over a sparse mid-scalp can look incongruous in ways that require planning around.
It affects the sessions discussion. Lower Norwood types can often be well-addressed in a single session that leaves meaningful donor supply for future needs. Higher Norwood types with large recipient areas require more explicit discussion of staged planning — what gets prioritized in the first session, what gets left for subsequent sessions, and how donor supply is managed across the patient’s likely lifetime of treatments.
It provides a framework for expectation-setting. Patients who understand their Norwood type can better evaluate what the procedure they’re considering can realistically achieve. A Type 6 patient who understands the scale knows they’re planning for comprehensive coverage of a large area with a necessarily limited donor supply — which requires different expectations than a Type 3 patient planning to address a relatively limited recession with good donor characteristics.
The Norwood Scale and Age: Why Type Alone Is Never Enough
One of the most important limitations of the Norwood scale as a planning tool is that it describes a patient’s current hair loss presentation without capturing where that patient is in their progression — which is clinically as important as where they currently are.
A 28-year-old presenting as Norwood Type 3 is in a fundamentally different clinical position from a 52-year-old presenting as Norwood Type 3. The 52-year-old at Type 3 may have reached or approached the natural endpoint of their pattern — their loss may have been stable for years and their future progression may be limited. The 28-year-old at Type 3 is almost certainly at an early stage of a pattern that will continue progressing — they may reach Type 5 or Type 6 over the following decade and beyond, even if they’re currently presenting at Type 3.
This distinction is critical for surgical planning because it determines how conservatively the procedure must be approached. The 52-year-old with stable Type 3 can be planned for comprehensively, with the current loss treated as close to the final picture. The 28-year-old with progressing Type 3 must be planned for against an unknown but likely substantially larger future pattern — which means conservative first-session design, explicit donor supply management, and careful discussion of what the result will look like not just at year one but at year ten.
Norwood type without age context, rate of progression, family history, and medical management status is an incomplete clinical picture. Every planning conversation must layer these additional variables over the baseline Norwood classification to produce a genuinely useful assessment of what the patient needs.
Family History and the Norwood Scale: Predicting Future Progression
Because androgenetic alopecia has a significant genetic component, family history provides useful — if imperfect — guidance about the likely trajectory of a patient’s hair loss. Examining the patterns in first-degree male relatives, particularly the father and maternal grandfather, gives a rough prediction of where the patient’s pattern may eventually progress.
A patient currently at Norwood Type 3 whose father and maternal grandfather both reached Type 6 is showing early stages of what is likely to be a significantly advanced eventual pattern. The surgical plan for this patient must account for the gap between their current Type 3 presentation and their probable eventual Type 5 or 6 — which has direct implications for how aggressively the first session addresses the current loss and how much donor supply is preserved for future needs.
Family history is not deterministic — genetics in polygenic conditions like androgenetic alopecia are complex, and some patients don’t follow the pattern established by relatives. But it is one of the most useful available indicators of likely progression trajectory, and it should be explicitly discussed in any consultation where the patient’s age and current type suggest that significant additional progression is possible.
The Norwood Scale and Medical Management
The Norwood type a patient eventually reaches is not fixed at birth — it represents the end point of a progression that can be meaningfully slowed through medical management. Finasteride and minoxidil, the established medical treatments for androgenetic hair loss, reduce the rate of progression and can maintain hair at earlier Norwood types for extended periods in patients who respond well to treatment.
This has direct relevance to surgical planning. A patient who is well-managed on finasteride and has shown minimal progression over several years has a different planning picture than a patient who has declined medical management and is progressing rapidly through Norwood types. The former can be planned more confidently as relatively stable; the latter requires more conservative surgical planning that accounts for likely continued rapid progression.
The practical implication for patients considering a hair transplant is that starting medical management before or around the time of the procedure — and maintaining it consistently afterward — is one of the most effective tools for managing the Norwood progression that will continue after the transplanted hair is established. The transplanted hair is permanent in its new location. The native hair continues to follow its genetic trajectory. Medical management that slows that trajectory preserves the native hair that provides context and surrounding coverage for the transplanted zone.
What the Norwood Scale Doesn’t Capture
As useful as the Norwood scale is as a communication tool and planning framework, experienced surgeons understand its limitations clearly — because planning based only on Norwood type, without accounting for what the scale misses, produces inadequate results.
Hair characteristics are not captured. Two patients at the same Norwood type can have dramatically different planning pictures depending on their hair caliber, texture, color, and the contrast between their hair and scalp. A patient with coarse, wavy, dark hair at Type 4 can achieve very different visual coverage from the same graft count as a patient with fine, straight, light hair at the same type. The Norwood type tells you how much area needs coverage — it tells you nothing about how much coverage a given graft count will provide in that area for that patient’s specific hair.
Donor area quality and quantity are not captured. The Norwood scale describes the recipient area — the zones of loss. It says nothing about the donor area — the resource available to address that loss. Two patients at the same Norwood type can have donor areas that differ substantially in density, scalp laxity, hair caliber, and the size of the permanent zone. These donor characteristics determine how many grafts are available across the patient’s lifetime, which is as important as knowing how many grafts the recipient area needs.
Diffuse thinning presentations are poorly described. The Norwood scale was designed to describe the most common pattern of male androgenetic alopecia, which progresses from defined recession zones and crown loss. Patients with diffuse thinning — where hair loss is generalized across the scalp rather than concentrated in specific recession patterns — don’t fit the Norwood framework well. Their clinical presentation requires different planning approaches than the Norwood-patterned presentations the scale was designed to describe.
Female pattern hair loss is not described. The Norwood scale applies to male pattern hair loss. Female androgenetic alopecia typically presents differently — with diffuse thinning across the crown and mid-scalp rather than the recession pattern characteristic of male loss — and is described by separate classification systems, primarily the Ludwig scale. Female patients evaluating hair transplant options should understand that the Norwood framework doesn’t apply to their presentation.
How Surgeons Use the Norwood Scale in Practice
In practice, experienced hair restoration surgeons use the Norwood classification as a starting point for the planning conversation rather than as a complete clinical assessment. The Norwood type locates the patient in the progression and provides a shared reference point for discussing coverage needs and planning priorities — and then the conversation immediately moves to the variables the scale doesn’t capture.
A thorough consultation at a quality clinic will establish the Norwood type and then build on it: assessing the donor area characteristics, discussing the patient’s age and likely progression trajectory, reviewing family history and medical management status, evaluating hair characteristics and what they imply for coverage per graft, and discussing what realistic goals look like given all these factors together.
The Norwood type is the beginning of this conversation, not its conclusion. A consultation that establishes the Norwood type and moves directly to graft count and pricing without working through the additional clinical variables is skipping the parts of the assessment that most directly determine whether the patient’s long-term interests are being served.
Using Your Norwood Type to Prepare for Consultation
Understanding your approximate Norwood type before a consultation is genuinely useful preparation — not because you’ll be doing the surgical planning, but because it gives you a framework for understanding what’s being discussed and a basis for asking informed questions.
If you’re at Norwood Type 2 or 3, the questions most relevant to your planning are about progression: how stable is your current pattern, what does your family history suggest about eventual pattern, and how does the surgical plan account for likely future progression rather than only current loss?
If you’re at Norwood Type 4 or 5, the questions most relevant to your planning are about prioritization and donor management: what gets addressed in the first session, what is left for future sessions, how much donor supply is preserved, and what will the overall coverage picture look like not just at year one but at year ten?
If you’re at Norwood Type 6 or 7, the most important questions are about honest expectations: what is realistically achievable with the available donor supply, what trade-offs are involved in the coverage plan, and what does a result that looks natural and intentional look like at this stage of loss?
At Hairpol, the Norwood classification is the starting point of every consultation — but only the starting point. The planning that follows incorporates the full clinical picture: donor characteristics, hair properties, age and progression trajectory, medical management, and the patient’s specific priorities and realistic goals. Because a plan built on Norwood type alone is a plan built on an incomplete picture, and incomplete planning produces results that look excellent at year one and increasingly inadequate at year five and beyond.
The Bottom Line
The Norwood scale is one of the most useful tools in the hair restoration clinician’s vocabulary — a shared language for describing hair loss patterns that allows efficient communication about coverage needs, planning priorities, and realistic expectations. Understanding your Norwood type gives you meaningful context for the consultation conversation and a framework for engaging with the planning process rather than simply receiving recommendations.
It is not, however, a complete clinical picture. The variables the scale doesn’t capture — hair characteristics, donor quality, age and progression trajectory, family history, medical management status — are as important to good surgical planning as the Norwood type itself. The best use of the Norwood scale is as an entry point to a comprehensive assessment rather than as a substitute for one.
Know your type. Ask the questions your type raises. And expect a consultation that goes substantially further than the scale alone can take you.
Frequently Asked Questions (FAQ)
What is the Norwood scale?
The Norwood scale — formally the Norwood-Hamilton scale — is the standard classification system used worldwide to describe the progression of male pattern androgenetic hair loss. It was originally developed by Dr. James Hamilton in the 1950s and revised by Dr. O'Tar Norwood in the 1970s, whose name it now carries. The scale runs from Type 1 (no significant hair loss, intact hairline) through Type 7 (extensive loss with only a narrow horseshoe of hair remaining at the back and sides of the scalp). Intermediate types — 2 through 6 — describe progressively advancing stages of recession and crown loss, with several types having variant classifications that capture presentations that don't fit the main sequence. The scale provides a shared vocabulary for surgeons, researchers, and patients to communicate about hair loss patterns and is the primary framework used in hair transplant planning consultations worldwide.
Why does my Norwood type matter for hair transplant planning?
Your Norwood type matters for hair transplant planning in several interconnected ways. It determines the total area of loss that needs to be addressed, which shapes the coverage conversation — how many grafts are needed, what zones require priority, and what is realistically achievable within the available donor supply. It informs hairline design decisions, since appropriate hairline position and coverage planning varies with the overall pattern of loss. It affects the sessions discussion — lower Norwood types can often be comprehensively addressed in a single session, while higher types require staged planning across multiple procedures with explicit donor management. And it provides the foundation for expectation-setting — a Type 2 patient and a Type 6 patient are having fundamentally different conversations about what a procedure can accomplish. Your Norwood type is the starting point of the surgical planning conversation, though experienced surgeons always build on it with additional clinical variables it doesn't capture.
What is the difference between Norwood Type 3 and Type 4?
Norwood Type 3 describes defined recession at the temples forming the characteristic M-shape associated with early significant hair loss, with the mid-scalp largely intact and crown loss absent or minimal. It is the most common stage at which patients present for their first hair transplant consultation. Norwood Type 4 represents more advanced progression — further frontal recession, more extensive temple loss, and clearly established crown thinning or loss. The mid-scalp bridge of retained hair that separates the frontal and crown loss zones is present in Type 4 but narrower than in Type 3. The surgical planning implications differ accordingly: Type 3 planning typically focuses primarily on the hairline and temples, while Type 4 planning must address both the frontal zone and the crown — a larger recipient area requiring more grafts and more complex prioritization decisions, particularly around how donor supply is allocated across both zones.
Can the Norwood scale predict how much hair loss I will eventually have?
The Norwood scale describes your current hair loss presentation — it does not predict your eventual pattern with certainty. However, combined with other clinical information, it provides useful context for planning around likely future progression. The most informative predictors of eventual pattern are family history — particularly the patterns of first-degree male relatives like father and maternal grandfather — and the rate of progression the patient has shown in the years leading to consultation. A patient currently at Norwood Type 3 whose close male relatives are Type 6 is showing early stages of what is likely to be a significantly advanced eventual pattern, which has direct implications for how conservatively the first hair transplant session should be planned. Medical management with finasteride or minoxidil can meaningfully slow progression, which also affects how the eventual pattern develops relative to what family history alone would suggest.
Does the Norwood scale apply to women?
No — the Norwood scale applies specifically to male pattern androgenetic hair loss and does not accurately describe the typical presentation of female hair loss. Female androgenetic alopecia generally presents differently from male pattern loss — typically as diffuse thinning across the crown and mid-scalp rather than the defined recession pattern that characterizes male loss and that the Norwood scale was designed to classify. Female pattern hair loss is more accurately described by the Ludwig scale, which runs from Ludwig Type 1 (mild diffuse thinning on the crown) through Type 3 (extensive crown thinning with preserved frontal hairline), or by the Sinclair scale. Women considering a hair transplant should be assessed using classification systems appropriate for female pattern loss rather than the Norwood framework, and the surgical planning considerations for female hair restoration differ significantly from those for male androgenetic alopecia.
What does Norwood Type 7 mean for hair transplant options?
Norwood Type 7 represents the most advanced stage of male pattern hair loss — extensive loss across the entire top of the scalp with only a narrow band of hair remaining at the back and sides. For hair transplant planning, Type 7 presents the most challenging relationship between recipient area size and available donor supply. The total area of loss is at its maximum, the permanent donor zone may be more limited than at earlier stages, and the gap between what would be needed for comprehensive coverage and what the donor supply can realistically provide is at its largest. This doesn't mean hair transplants are ineffective at Type 7 — meaningful and satisfying improvement is achievable — but the planning conversation must be very explicit about what is achievable within the available donor supply, what areas are prioritized for the highest visual impact per graft, and what realistic expectations include for comprehensive coverage of a very large area.
I'm 25 years old and Norwood Type 3. What should I know about hair transplant planning?
Being 25 and Norwood Type 3 is one of the situations that requires the most careful surgical planning — not because treatment is inappropriate, but because your current Type 3 presentation is almost certainly not your final pattern. At 25, hair loss progression typically continues for years or decades, and many patients who present at Type 3 in their mid-twenties reach Type 5 or Type 6 by their late thirties or forties. A hair transplant plan that treats only your current Type 3 loss without accounting for this likely future progression can deplete the donor supply needed to address that progression before your pattern has fully expressed itself. Responsible planning at this age involves a conservative first session addressing the highest-priority areas, explicit donor supply management preserving meaningful grafts for future sessions, consistent medical management with finasteride to slow progression, and a realistic discussion of how many sessions may be needed across your lifetime as the pattern develops. A consultation that moves directly from Type 3 to a comprehensive coverage plan without this progression conversation is not giving you the information you need.
What factors matter for hair transplant planning beyond Norwood type?
The Norwood scale is a useful starting point but describes only the recipient area — the zones of loss. Several equally important clinical variables are not captured by the scale and must be assessed in any thorough hair transplant planning consultation. Donor area characteristics — the density, quality, and size of the permanent zone — determine how many grafts are available across the patient's lifetime, which is as important as knowing how many are needed. Hair characteristics — caliber, texture, color, and the contrast between hair and scalp — determine how much visual coverage a given graft count will provide, which varies significantly between patients at the same Norwood type. Age and progression trajectory determine how conservatively the procedure must be planned to preserve options for future loss. Family history provides the best available indicator of where the pattern is likely to eventually progress. And medical management status affects how rapidly ongoing loss will progress around the transplanted zone. A complete planning assessment layers all these variables over the Norwood classification — the scale is where the conversation starts, not where it ends.
